Please feel free to use our e-mail back service.
Case:
The 26-year-old male patient was referred to our practice by his periodontologist. Ten years ago, the patient underwent orthodontic treatment with multi-bracket appliances alio loco. The final treatment result was secured by means of two twisted steel retainers. The patient has been feeling „a drawing pain on the front teeth“ of the lower jaw whenever he eats sweet, sour, cold, hot and spicy food for about six months. Therefore, he consulted his general dentist. She referred the patient to Dr. Gernhardt, Chief Resident, Department of Periodontics at Martin-Luther-University.
Diagnosis:
Intraroral diagnosis:
- Recession of the gingiva on tooth 32, lingual, by about 4 mm with exposed root cementum
- Slight vestibular tilt of the crown of tooth 32, with clearly visible and palpable lingual tilt of root 32
- Bonded retainer 33 – 43 intact
X-ray diagnosis:
- OPG: Shortening of tooth 32 shown in the OPG
- CBCT: Only 40 percent of the root of tooth 32 is still in the bone, the root apex is completely outside of the bone.

Fig. 1: Intraoral photo of the front – tooth 32 is slightly protruded

Fig. 2: Intraoral photo right – distocclusion by 1PB, retainer between 13 and 12 visible, 12 enamel aplasia

Fig. 3: Intraoral photo left – neutrocclusion, retainer between 13 and 12 visible

Fig. 4: Intraoral photo, lingual, after removal of the bonded retainer 33-43 – recession on the gingiva by about 4 mm

Fig. 5: OPG – Tooth 32 significantly shortened in representation due to tilt
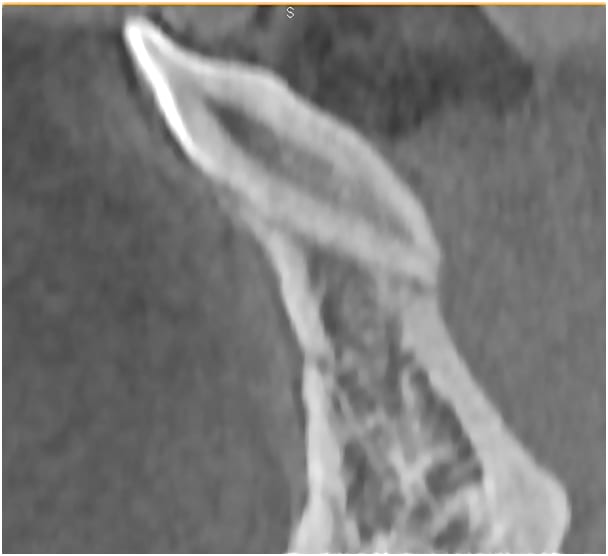
Fig. 6: Image generated from CBCT scan – tooth 32 markedly tilted, the lingual surface and root apex are not covered by bone
Therapy:
- Insertion of Forestadent 2D plus brackets to transmit torque so as to realign tooth 32
- A small tilted surface was adhered to tooth 32 in advance in order to compensate any torque losses caused by the bracket-wire system
- After 7 months, the bracket-wire system was fixed in place for another 6 months with a low-viscosity composite filling
- Insertion of a bonded retainer after 13 months of multi-bracket therapy (lingual)
- Dr. Gernhardt is responsible for covering the gingiva defect

Fig. 7: Intraoral photo taken at the end of the active treatment – multi-bracket system (2D plus – Forestadent) fixed with low-viscosity composite filling

Fig. 8: Intraoral photo taken after removal of the bonded bracket – the tilted surface on tooth 32 is clearly visible

Fig. 9: Intraoral photo – bonded retainer 33 - 43

Fig. 10: Intraoral photo taken with mirror by Dr. Gernhardt ZZMK Halle – status before the gingiva defect on 32 was covered
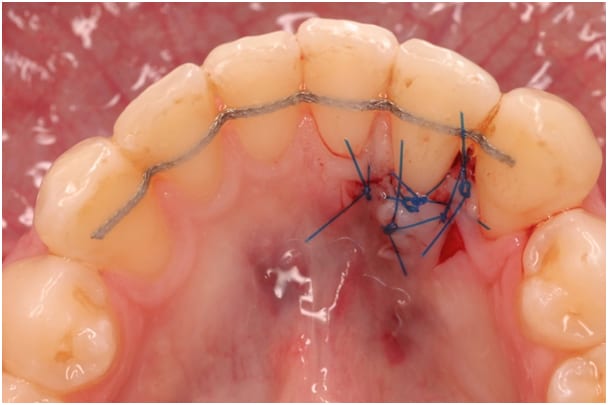
Fig. 11: Intraoral photo taken with mirror by Dr. Gernhardt ZZMK Halle – status after the gingiva defect on 32 was covered
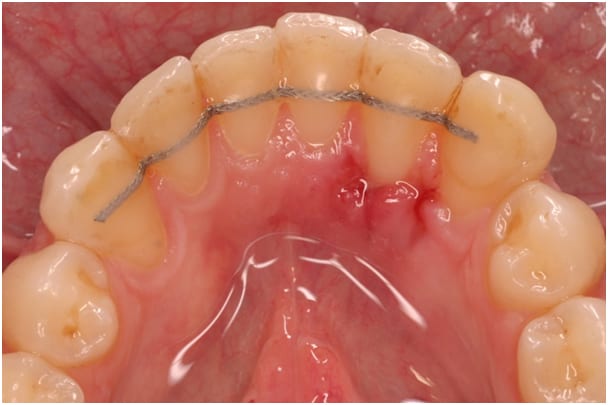
Fig. 12: Intraoral photo taken with mirror by Dr. Gernhardt ZZMK Halle – status after the suture removal (10d after the operation)

Fig. 13: Intraoral photo taken with mirror by Dr. Gernhardt ZZMK Halle – status 6 months after the operation
Epicrisis:
Following partial multi-bracket therapy, it was possible to align the completely exposed tooth 32 and root in the row of teeth again. Since the gingiva defect was covered by periodontal surgery, bone surrounded the defect determined with X-ray scans. The patient no longer experiences discomfort when eating.
Goal due to CBCT technology:
Tooth 32 could not have been reintegrated as precisely as it was without CBCT technology. It was only possible to formulate a systematic therapy concept with lingual partial multi-brackets because the exact location of the tooth was known. The CBCT scan taken at the end of the treatment shows the precise work of the multi-bracket appliances as well as the quality and skill of the periodontal surgery, since root 32, which was completely exposed, is surrounded by bone again.



